Last updated on Aug 5, 2026
United Behavioral Health Outpatient Treatment Progress free printable template
pdfFiller is not affiliated with any government organization
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is United Behavioral Health Outpatient Treatment Progress
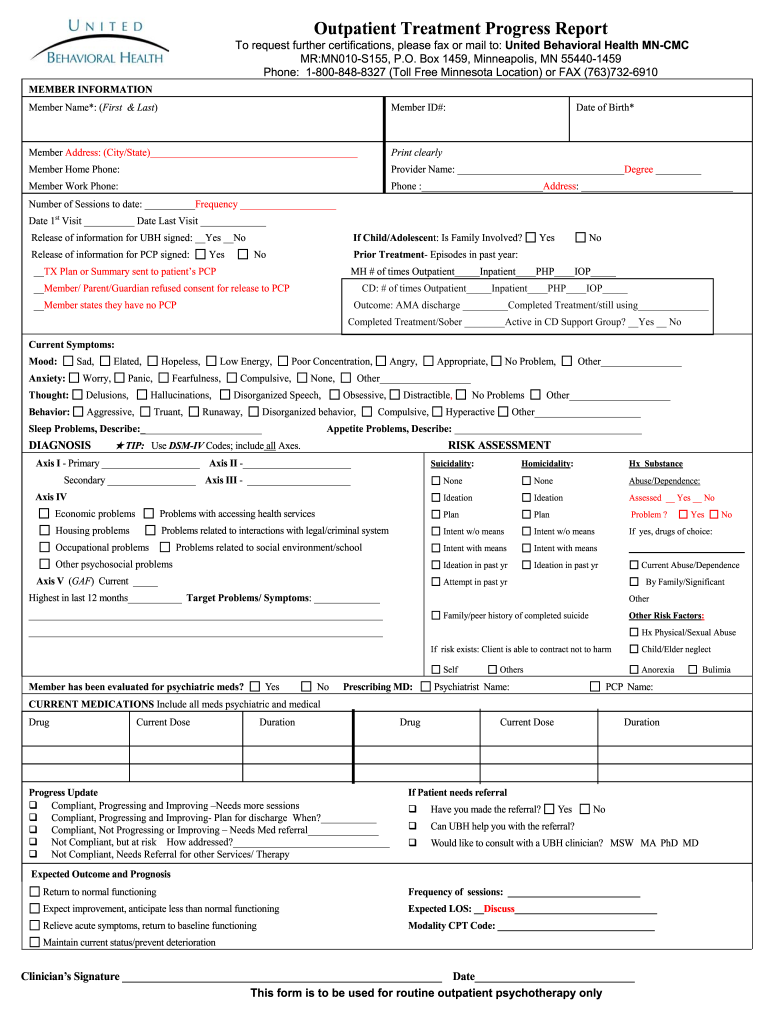
The Outpatient Treatment Progress Report is a healthcare form used by clinicians to document patient progress in outpatient psychotherapy.
pdfFiller scores top ratings on review platforms
I really like the fact rhat PDF filller allows me to work on very important PDF documents that I need to fill out but I still have trouble navigating these documents which is why I only gave 4 stars. Maybe with better instructiins...
I have used PDFfiller to fill out PDF forms which wow dave required my either purchasing a piece of software or otherwise some other form of complex document manipulation - PDFfiller has made PDF document handling a breeze for me.
Who needs United Behavioral Health Outpatient Treatment Progress?
Explore how professionals across industries use pdfFiller.

United Behavioral Health Outpatient Treatment Progress is needed by:
-
Mental health professionals
-
Psychotherapists providing outpatient care
-
Healthcare administrators overseeing patient records
-
Insurance companies requiring progress documentation
-
Patients receiving outpatient treatment
-
Clinical researchers tracking treatment efficacy
Comprehensive Guide to United Behavioral Health Outpatient Treatment Progress
What is the Outpatient Treatment Progress Report?
The Outpatient Treatment Progress Report is a vital tool designed for healthcare providers to effectively document the journey of a patient undergoing outpatient psychotherapy. This form is instrumental in accurately tracking a patient's progress, focusing on critical data such as member information, current symptoms, diagnosis, and progress updates. Essential sections include comprehensive fields for personal details and treatment specifics which facilitate detailed record-keeping.
Purpose and Benefits of the Outpatient Treatment Progress Report
This form serves an essential role within the healthcare process by enabling clinicians to meticulously track patient development. By documenting progress in an organized manner, healthcare professionals can make informed treatment decisions that enhance patient outcomes. Additionally, thorough documentation not only supports optimal patient care but also ensures legal compliance, safeguarding both patient and provider interests.
Key Features of the Outpatient Treatment Progress Report
The report boasts several important components and functionalities aimed at streamlining the documentation process. Key features include:
-
Fillable fields for capturing member details and symptoms.
-
Checkboxes that simplify responses for specific areas.
-
Clinician signatures required to authenticate the report.
-
A flexible structure to meet diverse patient case requirements.
These characteristics not only enhance the usability of the form but also contribute to its validity and effectiveness in medical record-keeping.
Who Needs the Outpatient Treatment Progress Report?
The Outpatient Treatment Progress Report is utilized by a variety of professionals, including clinicians, mental health practitioners, and other healthcare providers. It becomes particularly crucial in scenarios where documenting patient treatment is necessary for coordinated care. Patients also benefit from such structured documentation, as it fosters improved care coordination among their healthcare teams.
How to Fill Out the Outpatient Treatment Progress Report Online
Completing the Outpatient Treatment Progress Report online can be accomplished efficiently with a step-by-step approach using pdfFiller. Here’s how to proceed:
-
Gather necessary information, including member details and current symptoms.
-
Access the form on pdfFiller and begin filling in mandatory fields.
-
Utilize the tools to input detailed progress updates.
-
Review all information for accuracy before submission.
Accurate completion of each section is essential to uphold the integrity of the report.
Common Errors and How to Avoid Them When Completing the Outpatient Treatment Progress Report
When filling out the Outpatient Treatment Progress Report, certain pitfalls can arise. Frequent errors include:
-
Incomplete sections that leave critical information unrecorded.
-
Invalid information, which can lead to complications in treatment tracking.
To mitigate these issues, implement best practices such as conducting a thorough review and using a validation checklist to ensure all required fields are completed accurately before final submission.
Submission Methods for the Outpatient Treatment Progress Report
Submitting the completed Outpatient Treatment Progress Report is straightforward, with options available for both electronic and paper submission. Key details to consider include:
-
The preferred submission method—either electronically through pdfFiller or as a printed document.
-
Specific requirements based on the chosen submission route.
-
Processing times, giving insight into what to expect post-submission.
Understanding these methods streamlines the submission process and aids in timely treatment documentation.
Security and Compliance for the Outpatient Treatment Progress Report
Ensuring the security and compliance of the Outpatient Treatment Progress Report is paramount. pdfFiller employs robust measures to safeguard documents during handling and storage. Key points include adherence to:
-
HIPAA regulations to protect patient privacy.
-
GDPR compliance, emphasizing data protection standards.
These security protocols play a crucial role in maintaining patient confidentiality and secure transmission of sensitive healthcare information.
Using pdfFiller to Complete Your Outpatient Treatment Progress Report
pdfFiller enhances the process of completing the Outpatient Treatment Progress Report with its user-friendly features. Users can take advantage of:
-
Editing options that allow customization of content.
-
eSigning capabilities to confirm document authenticity.
The platform is designed to support efficient form management, making the documentation process smoother and more effective for healthcare providers.
Experience Seamless Document Management with pdfFiller
Users are encouraged to explore pdfFiller for creating, editing, and submitting their Outpatient Treatment Progress Reports. Efficient documentation is pivotal for enhancing patient care and optimizing clinician workflows, and pdfFiller provides a secure environment for managing sensitive medical documents effectively.
How to fill out the United Behavioral Health Outpatient Treatment Progress
-
1.To access the Outpatient Treatment Progress Report on pdfFiller, navigate to the website and use the search bar to find the form by its name.
-
2.Once the form appears, click on it to open the document in the pdfFiller interface for editing.
-
3.Before filling out the form, gather essential information such as the member's name, ID number, date of birth, current symptoms, and medications.
-
4.Start filling in the member information fields, ensuring accuracy to prevent future discrepancies.
-
5.Utilize the checkboxes and blank lines within the form to indicate symptoms, risks, and updates effectively; these elements guide the clinician in providing comprehensive information.
-
6.After completing all necessary sections, review the document for clarity and completeness.
-
7.Pay special attention to the clinician’s signature area, ensuring the authorized person signs before finalization.
-
8.To save the completed form, click 'Save' on the toolbar; you can also choose to download it directly to your device or send it to your email.
-
9.If needed, submit the form to the appropriate entity or directly through pdfFiller's submission options.
Who is eligible to fill out the Outpatient Treatment Progress Report?
The form must be filled out by licensed clinicians who are providing outpatient psychotherapy services to patients. This implies the need for proper credentials and training in mental health treatment.
Are there any deadlines for submitting the Outpatient Treatment Progress Report?
While specific deadlines may vary based on the provider or insurance requirements, it's advisable to submit the report as soon as the patient's session is concluded. This ensures up-to-date records are maintained.
What methods can be used to submit the filled Outpatient Treatment Progress Report?
You can submit the completed report electronically through pdfFiller by sending it to a designated email or printing and mailing it to the relevant office. Ensure to follow your organization’s submission protocols.
What supporting documents are needed with the Outpatient Treatment Progress Report?
Generally, no additional documents are required when submitting the report. However, check with your organization or insurance company, as they may ask for prior therapy notes or patient consent forms.
What common mistakes should be avoided when filling out this form?
Ensure all sections are accurately filled out, particularly the member’s information and clinician’s signature. Double-check for any omitted fields which could delay processing or cause issues.
What is the expected processing time once the Outpatient Treatment Progress Report is submitted?
Processing times may vary based on the receiving entity's workload. Typically, you can expect acknowledgment within a week; however, longer periods may occur during peak seasons or for complex cases.
Can patients access and review their Outpatient Treatment Progress Reports?
Yes, patients have the right to request their records, including the Outpatient Treatment Progress Report. Clinicians should provide this upon request, adhering to privacy regulations.
Related Content
Related Forms



Related Catalogs

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.